What Is a Macular Hole and How Does It Develop?
18/05/2026

04/05/2026
An epiretinal membrane (ERM), often referred to by patients as a macular pucker, is a thin layer of scar tissue that develops on the inner surface of the retina, over the macula. Although it may sound alarming, this is a relatively common retinal condition, particularly with age. In many cases it remains mild and stable, but in others it can lead to progressive visual distortion, reduced reading ability, and persistent blurry vision that begins to interfere with daily life.
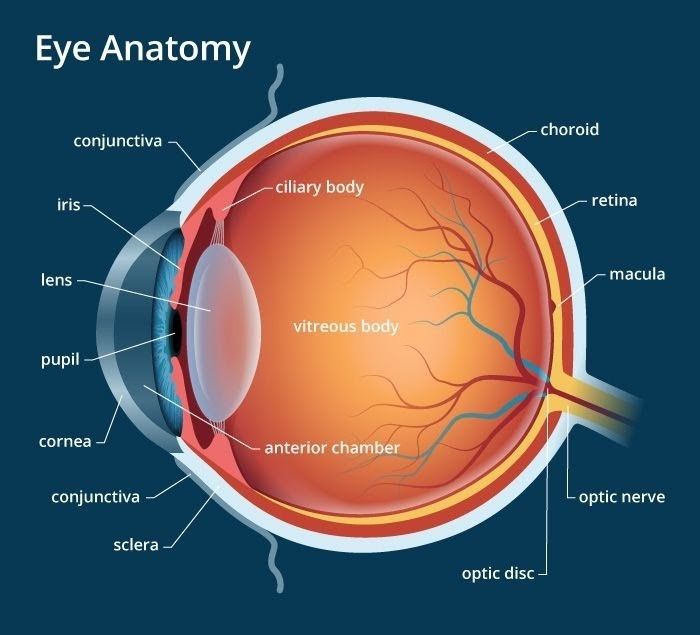
The macula is the central part of the retina responsible for detailed vision. It allows us to read, recognise faces, drive, and perform fine visual tasks. When a membrane forms on its surface, it can contract over time, creating traction. That traction may wrinkle or distort the macula, which explains why patients often describe straight lines as wavy, letters as uneven, or objects as appearing larger or smaller in one eye compared with the other.
From a clinical perspective, epiretinal membrane is not a single uniform disease. Some membranes are idiopathic, meaning they develop without a clear underlying retinal disorder and are commonly associated with posterior vitreous detachment and age-related changes at the vitreoretinal interface. Others are secondary to ocular conditions such as retinal tears, retinal detachment, diabetes, vascular occlusions, inflammation, trauma, or prior intraocular surgery. This distinction matters, because the behaviour of the membrane, the likelihood of progression, and the visual prognosis may differ depending on the cause.
Patients do not always notice symptoms in the early stages. A mild ERM may be picked up incidentally during a routine retinal examination or OCT scan. Once the membrane becomes more contractile, however, symptoms typically become more apparent. The most common complaints include blurry vision, metamorphopsia, reduced contrast sensitivity, difficulty with reading, monocular diplopia, and the sense that vision is “not crisp” despite an updated glasses prescription. Visual acuity may remain reasonably good while quality of vision is already noticeably impaired, which is why the patient’s functional complaints should always be taken seriously rather than judged on letter score alone.
Modern diagnosis relies heavily on optical coherence tomography. OCT has transformed the assessment of epiretinal membrane by allowing precise, cross-sectional imaging of the macula. It shows the presence of the membrane, the degree of retinal surface wrinkling, central retinal thickening, distortion of the foveal contour, and in some cases associated intraretinal cystic change or disruption of the outer retinal layers. These structural details are not merely descriptive; they help explain symptoms, guide timing of intervention, and support counselling regarding expected recovery.
Management depends on the severity of symptoms, the OCT findings, and the impact on the patient’s daily function. Not every epiretinal membrane requires immediate intervention. In fact, observation remains entirely appropriate for many patients with good visual function, mild distortion, and stable anatomy. A careful follow-up strategy is often the best first step, especially when the membrane is mild and the patient is coping well. It is important to remember that surgery is performed to improve meaningful visual function, not simply to treat an OCT image.
That said, there comes a point when observation is no longer enough. When patients develop worsening distortion, increasing difficulty with reading or driving, or progressive decline in visual acuity, surgery becomes a reasonable and often very effective option. The standard treatment is pars plana vitrectomy with membrane removal, usually combined with internal limiting membrane peeling to reduce the risk of recurrence. In the setting of retina surgery, as in other advanced vitreoretinal centres worldwide, this is a well-established microsurgical procedure performed with modern small-gauge instrumentation and high-resolution intraoperative visualisation.
The principle of surgery is straightforward, even if the technique is highly specialised. The vitreous is removed, access to the retinal surface is obtained, and the epiretinal membrane is delicately peeled away from the macula using fine forceps. In many cases, a dye is used to assist visualisation of the internal limiting membrane, which is then peeled as well. This additional step can improve the anatomical result and lower recurrence rates, though it must be performed with sound surgical judgement and gentle technique.
Patient counselling before surgery is crucial. The goal of membrane removal is usually to reduce distortion and improve the quality of central vision, but recovery is not immediate. Vision often improves gradually over weeks to months, and the extent of recovery depends on several factors: duration of symptoms, preoperative visual acuity, degree of macular distortion, integrity of the photoreceptor layers, and the presence of coexisting ocular disease such as cataract or glaucoma. Patients with long-standing traction may improve meaningfully yet still not return to completely normal vision. Setting realistic expectations is therefore just as important as performing the procedure well.
One of the most common questions in clinic is timing. Should surgery be done early, or is it better to wait until vision is significantly reduced? There is no single threshold that applies to every patient. Some individuals tolerate mild blur but are greatly affected by distortion. Others may read the chart relatively well yet struggle with professional or visually demanding tasks. In practice, the decision is individualised. It should take into account symptoms, occupation, OCT progression, binocular visual function, and the patient’s own priorities. Surgery should not be delayed so long that chronic structural damage limits recovery, but it should also not be rushed in an eye that remains stable and minimally symptomatic.
When symptoms begin to limit quality of life, membrane removal through vitrectomy can be an excellent option. In experienced retinal centres offering retina surgery, the combination of precise diagnosis, modern surgical technique, and realistic patient counselling allows for consistently strong care. The best results come from understanding not only what the membrane looks like, but how it is affecting the person behind the scan.
Email: appointments@barraquer.ae
Phone (outside UAE): +971 4 573 9999
Toll-Free (inside UAE): 800 234 823 (BEHUAE)
Working Hours & Location: Click on Google Map Link