
24/04/2026
There are few ophthalmic emergencies more time-sensitive than a retinal detachment. Patients often describe the first symptoms in deceptively mild terms: a sudden increase in floaters, brief flashes of light, or the sensation that a dark shadow is moving across part of the visual field. These symptoms may be painless, but they should never be dismissed. In the appropriate clinical context, they may indicate a retinal tear progressing to retinal detachment, a condition in which prompt diagnosis and treatment are critical to preserving sight.
At Barraquer Eye Hospital, patients presenting with these warning signs are evaluated urgently, because retinal detachment is not a condition that allows for delay. The retina is a highly specialized neurosensory tissue lining the back of the eye. Once it separates from the underlying retinal pigment epithelium and choroidal blood supply, its function begins to deteriorate. The longer the detachment persists, the greater the risk of permanent visual loss.
This is why retinal detachment surgery must often be approached as retina emergency surgery. The goal is not simply anatomical repair, but restoration of retinal attachment before irreversible damage occurs.
Recognizing the early signs
In clinical practice, the presenting symptoms are often remarkably consistent. Patients may notice:
- a sudden onset or marked increase in floaters
- flashes of light, particularly in peripheral vision
- distortion or blurring of vision
- a curtain-like or shadow-like defect spreading across the field of vision
These symptoms reflect traction on the retina, retinal tearing, or extension of subretinal fluid. Although not every patient with floaters or flashes has a retinal detachment, every patient with acute-onset symptoms should be evaluated promptly by an ophthalmologist, ideally one with access to retinal imaging and vitreoretinal surgical care.
A representative patient at Barraquer Eye Hospital described the experience in the following way:
"It started with a few new floaters, like tiny spots drifting across my vision. A little later I began to notice flashes, especially when I moved my eyes. Then a dark shadow started coming across one side of my vision. Because I already knew the team at Barraquer Eye Hospital, I came in straight away. They examined me immediately and confirmed that I had a retinal detachment. I had prompt surgery, and my vision returned to normal. Acting quickly helped me avoid blindness."
This account captures the essential point: the outcome in retinal detachment often depends on how quickly the patient presents and how rapidly treatment can be organized.
Why retinal detachment is a true emergency
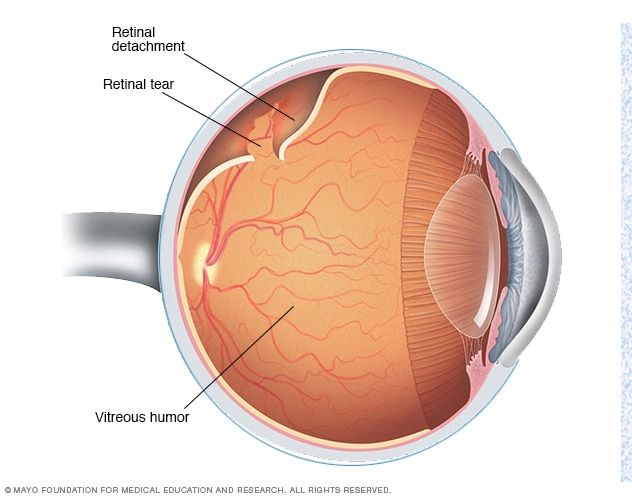
Retinal detachment is not a uniform entity. The most common type is rhegmatogenous retinal detachment, which occurs when a retinal break allows liquefied vitreous to pass into the subretinal space, separating the neurosensory retina from the underlying tissue. Less commonly, detachments may be tractional or exudative, each with distinct mechanisms and management considerations.
From a prognostic standpoint, one of the most important clinical distinctions is whether the macula remains attached. In a so-called “macula-on” detachment, central vision is still preserved at presentation, and urgent surgery aims to maintain that function. In a “macula-off” detachment, central vision has already been affected, and although surgery remains necessary, postoperative visual recovery is often less complete.
For this reason, the timing of retina repair is central to outcome. A patient who presents early, before macular involvement, has a substantially better chance of regaining excellent functional vision than one who presents late.
Surgical principles of retina repair
Modern retina repair is highly specialized and tailored to the configuration of the detachment, the location and number of retinal breaks, lens status, age of the patient, vitreous status, and the presence or absence of proliferative vitreoretinopathy. The two principal surgical techniques remain vitrectomy and scleral buckle, used either individually or in combination depending on the case.
Vitrectomy
Pars plana vitrectomy has become the dominant approach for many forms of retinal detachment, particularly in pseudophakic eyes, in complex detachments, or when media opacity limits visualization. During vitrectomy, the vitreous gel is removed, traction on the retina is relieved, retinal breaks are identified and treated with endolaser or cryotherapy, and an internal tamponade agent such as expansile gas or silicone oil is introduced to stabilize the retina during healing.
Vitrectomy offers important advantages. It allows direct management of vitreoretinal traction, improves access to posterior pathology, and is particularly useful when multiple breaks, giant retinal tears, vitreous hemorrhage, or early proliferative vitreoretinopathy are present. It has therefore become central to contemporary retinal detachment surgery in Dubai, particularly in tertiary referral settings.
Scleral buckle
The scleral buckle remains a well-established and highly effective procedure in appropriately selected patients. In this technique, a silicone element is placed externally on the sclera to indent the wall of the eye, thereby reducing vitreoretinal traction and supporting closure of the retinal break. Cryotherapy or laser retinopexy is typically used to secure the break.
Although sometimes regarded as a more traditional operation, scleral buckle continues to play an important role, particularly in younger patients with uncomplicated rhegmatogenous retinal detachment and well-defined peripheral breaks. In experienced hands, it offers durable anatomical success and can be especially valuable when the aim is to avoid entering the vitreous cavity.
Combined scleral buckle and vitrectomy
In selected cases, the most effective strategy is a combined procedure using scleral buckle and vitrectomy together. This may be appropriate in more complex detachments, in inferior retinal breaks, in extensive pathology, or when the surgeon judges that both internal and external support will improve the likelihood of long-term reattachment.
At Barraquer Eye Hospital, surgical planning is individualized. The choice of procedure is based on retinal findings rather than a fixed protocol, which is an important principle in vitreoretinal practice.
What patients can expect
Although a retinal emergency, management is usually structured. After diagnosis, the retina specialist explains the condition, assesses urgency, and proceeds with surgery under local or general anesthesia as appropriate.
Vitrectomy patients require counselling on gas tamponade, which necessitates postoperative positioning and avoidance of air travel until fully absorbed due to pressure risk.
Vision is typically blurred initially, especially with a gas bubble. Mild discomfort is expected, while significant pain should be reviewed. Visual outcomes depend mainly on detachment duration and macular involvement
Outcomes and prognosis
The primary anatomical success rate of modern retinal detachment surgery is high, and many patients achieve reattachment after a single procedure. Functional outcome, however, is influenced by more than anatomical success alone. Even with technically successful surgery, final visual acuity may be limited by macular detachment, chronicity of the condition, proliferative vitreoretinopathy, coexisting cataract, or pre-existing retinal disease.
That said, early diagnosis and timely intervention substantially improve the likelihood of a favorable result. The patient testimonial above illustrates the best-case clinical pathway: recognition of symptoms, immediate presentation, prompt confirmation of the diagnosis, and rapid surgery before irreversible damage developed. In such cases, return to near-normal or normal vision is entirely possible.
Why quick access matters
The strength of a retina service lies not only in surgical expertise, but in access. A patient with acute symptoms should not face unnecessary delays between first presentation, retinal examination, imaging, surgical decision-making, and operative treatment. In this respect, centers such as Barraquer Eye Hospital play an important role in providing streamlined assessment and timely vitreoretinal care for patients requiring retinal detachment surgery in Dubai.
For patients, the message is simple but important: sudden floaters, flashes, and a dark peripheral shadow are not symptoms to “watch and wait.” They warrant urgent evaluation. For clinicians, the principle remains equally clear: retinal detachment is a sight-threatening emergency in which time is a major determinant of outcome.
Final perspective
Retinal detachment remains one of the clearest examples in ophthalmology recognition of a condition in which prompt alters prognosis. The warning signs are often subtle, but the underlying pathology is potentially devastating if untreated. Fortunately, modern retina repair techniques, including vitrectomy and scleral buckle, offer highly effective treatment when applied in a timely and appropriate manner.
At Barraquer Eye Hospital, the emphasis is on exactly that: early diagnosis, rapid intervention, and individualized surgical management. For the patient who presents in time, the difference can be profound, not only in anatomical repair of the retina, but in preservation of useful vision and avoidance of permanent blindness.
Schedule a consultation today
-
Email: appointments@barraquer.ae
-
Phone (outside UAE): +971 4 573 9999
-
Toll-Free (inside UAE): 800 234 823 (BEHUAE)
-
Working Hours & Location : Click on Google Map Link